Welcome
Fungi are everywhere around us; they are the most abundant form of life on the planet, counting about 12 million species worldwide. Only a small fraction of them cause disease in humans, but they are responsible for about a billion infections each year.
News & Features
Educational Programs
Case of the month
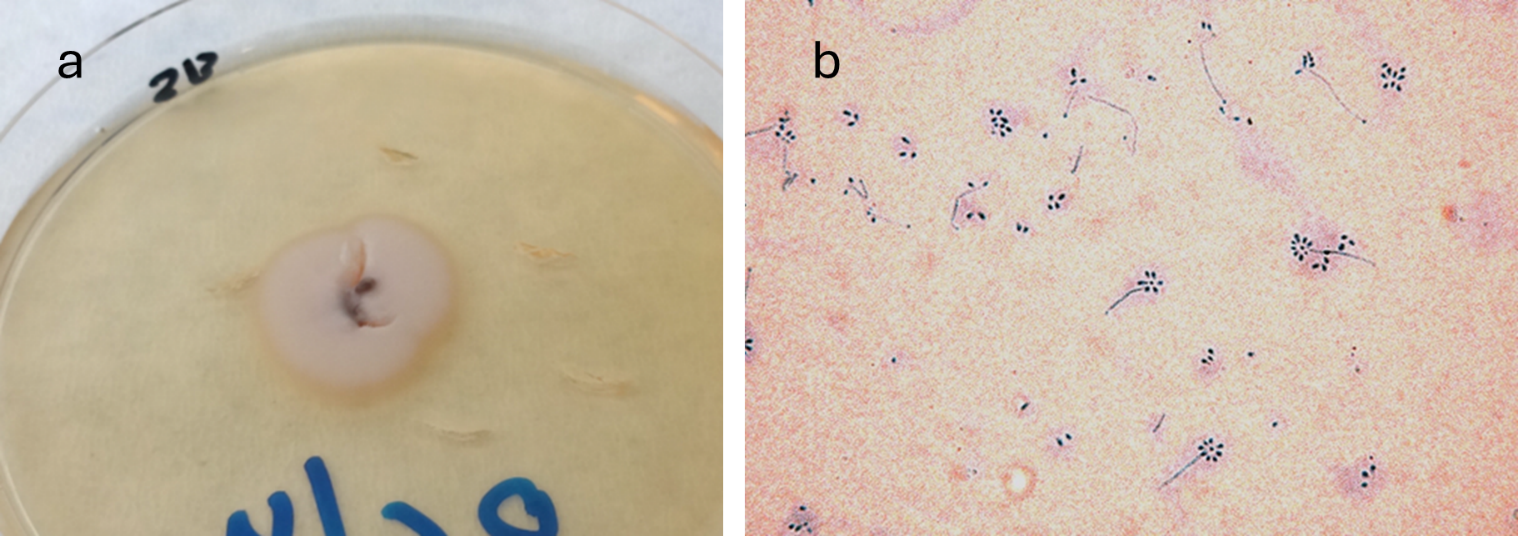
a) Colony on Sabouraud agar (5 days, 25 °C); b) microscopic morphology of the colony with lactophenol cotton blue stain, x400 magnification
(Photos: Miranda Drogari-Apiranthitou, Infectious Diseases Research Laboratory, 4th Dept of Internal Medicine, National and Kapodistrian University of Athens)
Read more
A 22-year-old man presented to the outpatient clinic of a Greek hospital with painless nodular ulcerated lesions and regional lymphadenitis on the right lateral neck. The lesions began as a small painless nodule three months earlier during travel to Colombia, where he worked on coffee plantations. After returning to Greece, additional nodular lesions appeared in the same area, following the superficial lymphatic drainage. He did not recall any trauma or abrasion. He had no systemic symptoms, had received no treatment, and his medical history was unremarkable.
Culture of skin scrapings on Sabouraud agar at 25 °C resulted in growth of a filamentous fungus (mold) forming a characteristic creamy colony after 5 days of incubation. The same fungus grew from a subsequent skin tissue biopsy culture. After 7 days of incubation in brain-heart infusion broth at 37 °C, the organism converted to a yeast form.
Based on the colony morphology on Sabouraud agar at 25 °C (a) and the microscopic appearance (b), which fungal species is most likely?
- Acremonium kiliense
- Sporothrix schenkii
- Talaromyces marneffei
- Scedosporium apiospermum


Events (co) organized/financially supported by the HSoMM
Publications
New interesting articles
Fungi are everywhere around us; they are the most abundant form of life on the planet, counting about 12 million species worldwide. Only a small fraction of them cause disease in humans, but they are responsible for about a billion infections each year. At the same time, new fungi pathogenic to humans are emerging (such as Candida auris, the azole-resistant Aspergillus fumigatus, etc.) due to climate change and new environmental conditions.
Fungal infections are responsible for more than 1.5 million deaths each year, mostly in immunocompromised patients, while affecting the lives of many millions more. However, they remain a neglected topic by public health authorities, even though most deaths from fungal infections are preventable. It was not until October 2022 that the World Health Organization published the first list of priority fungal pathogens, to increase global interest in the infections they cause and their resistance to antifungal drugs.
The aims of the HSoMM are:
- The promotion of Medical Mycology in Greece and abroad.
- The encouragement and reinforcement of all research efforts and studies in Greece regarding prevention, diagnosis, and treatment of fungal infections.
- The collaboration with public and private institutions and organizations in Greece and abroad, for the progress of Medical Mycology.